CEREBRAL PALSY
Cerebral palsy (CP) is a lifelong condition that affects the individual, family, and immediate community. It is a childhood condition in which there is a motor disability (palsy) caused by a static, non-progressive lesion in the brain.
The causative event has to occur in early childhood, usually defined as less than 2 years of age. Children with CP have a condition that is stable and non- progressive; therefore, they are in most ways normal children with special needs.
The goal of having a concept of motor control is to help in treatment of children with motor control problems. When considering individual pathological problems, the neurological aspects of the motor impairments can be separated into abnormalities of the three subsystems of motor control. These subsystems are muscle tone, motor planning, and balance.The variety of abnormalities in these three subsystems leads to almost all the motor problems in children with CP.
In my succeeding blogs, I will be writing about Cerebral palsy and problems related to it. In this blog i would like to give a brief information about the medications like BOTOX (Botlinum toxin), Phenol and local anesthetics in controlling SPASTICITY which is a tonal abnormality.
TONE :
TONE is defined as the resistance of muscle to passive elongation or stretch when an individual attempts muscle relaxation. It is due to a. physical inertia; b. intrinsic mechanical-elastic stiffness of muscle and connective tissues and c. reflex muscle contraction. Disorders of Muscle Tone: Tonal abnormalities are categorized as hypertonia (increased above normal resting levels), hypotonia (decreased below normal resting levels) or dystonia (impaired or disordered tonicity).
Spasticity: Spasticity is the most common presentation of all neurological alterations in children with CP. It is a hypertonic motor disorder characterized by velocity-dependent resistance to passive stretch. Symptoms such as clonus, hyperactive tendon reflexes, and spasms are included within the umbrella term ‘spasticity’. It occurs as a part of UPPER MOTOR NEURON (UMN) syndrome as injury to the pyramidal tracts (corticospinal pathways). The signs and symptoms of UMN syndrome includes:
| Clonus |
| Spasms |
| Mass reflex responses (exaggerated cutaneous and autonomic responses, flexor reflex afferents) |
| Pathological reflexes (e.g Babinski’s and Hoffman) |
| UMN SYNDROME RESULTS IN | |||
|
|||
Measuring Muscle Tone:
A. Clinical measures : Range of motion, Modified Ashworth Scale , Tardieu Scale
Modified Ashworth Scale:
00 Hypotonia
0 Normal tone, no increase in tone
1 Slight increase in tone manifested by a slight catch and release or minimal increased resistance to joint range of motion.
1+ Slight increase in tone manifested by a slight catch and minimal increased resistance to joint range of motion for more than half the joint range.
2 More marked increase of tone through most of the whole joint range, but the affected joint is easily moved.
3 Considerable increase in muscle tone; passive movement difficult but possible
4 Affected joint is stiff and cannot be moved
B. Mechanical instruments: The pendulum test
C. Electrophysiological measures: The H reflex, Vibration inhibition index
D. Functional measures: Upper extremity function, Gait.
EFFECTS OF SPASTICITY
Positive effects
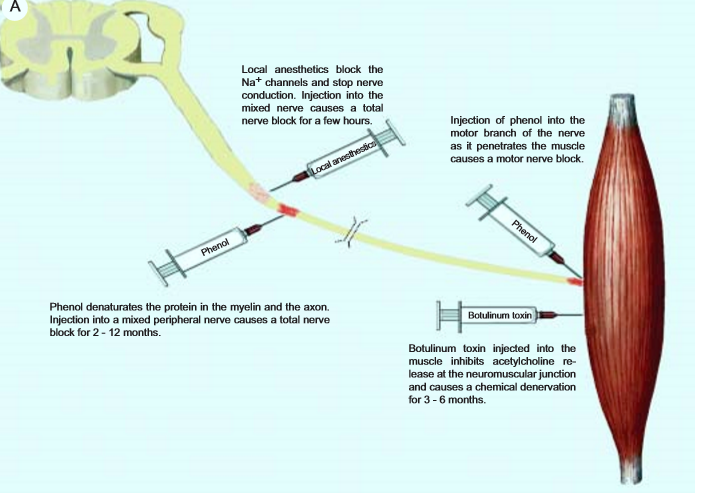
- These block nerve conduction by changing membrane permeability to sodium ions. They affect both sensory and motor function in the area innervated by the nerve. This effect is completely reversible and causes no structural damage to the nerve.
- The effect starts within 3-15 minutes after the injection and lasts from 45 minutes to 8-12 hours depending on the type of drug used. Median nerve in the upper extremity and many nerves in the lower extremity are available for local anesthetic blocks. (like; Tibial, Obturator, Femoral ,Sciatic blocks).
- Local anesthetic blocks may be used as a diagnostic tool to differentiate spasticity from contracture and to predict functional changes with long term therapy.
Advantages of local anesthetic blocks:
- Reversible short duration effect.
- Relatively painless.
- Helps differentiate contracture from spasticity.
- Unmasks activity in the antagonists by relaxing the spastic muscles.
Side effects and precautions:
- Hypersensitivity reaction.
- Hematoma at injection site.
- Sudden weakness may cause injuries in the unprepared patient.
- Systemic toxicity (dose related).
Chemical neurolysis: alcohol and phenol
- It causes protein denaturation and non-selective tissue destruction in the injected area. Wallerian degeneration of neurons occurs in the weeks following injection. Most axons regrow, over a period of time.
- The effect of phenol starts rapidly because of its local anesthetic properties and lasts for up to 2 to 12 months.
- The rectus femoris motor point block.
- The hamstring motor point block.
- Adductor muscle motor point block.
- Tibial nerve block.
- Rapid action
- Longer duration
- Low cost
- No antibody formation
- Relatively painful injection
- Chronic dysesthesia and pain
- Peripheral edema, deep venous thrombosis
- Reversible sensory loss
- Systemic side effects (dose related)
- Relatively difficult technique
BOTULINUM TOXIN
- §The toxin must enter the nerve endings to exert its effect. It becomes fully active once inside the cholinergic nerve terminal.
- §When the impulse for contraction arrives at the axon terminal acetylcholine (Ach) vesicles fuse with the nerve membrane and the Ach is released into the synaptic cleft. This causes excitation in the muscle fiber and muscle contraction.
- §The various serotypes of botulinum toxin act on different portions of the acetylcholine vesicle complex. Botulinum toxin inhibits the fusion of acetylcholine vesicles at the pre-synaptic membrane.
- §Ach cannot be released into the synaptic cleft, the impulse from the nerve to the muscle fiber is blocked and the muscle fibers innervated by that axon cannot contract. This is chemical denervation.
- §The extent of muscle weakness created by the botulinum toxin depends on the serotype, dose and volume of toxin used.
- §The effect of botulinum toxin is reversible. Nerve sprouts form at the unmyelinated terminal axon immediately proximal to the end plate.
- § These sprouts innervate the muscle fiber. Eventually, the original neuromuscular junction regains function .
- §This terminates the clinical effect in 3 – 6 months and spasticity reappears.
- §To improve walking in the spastic diplegic and hemiplegic child.
- §To minimise adductor tone in the child with early hip subluxation.
- §To decrease the spasms and pain in the spastic-athetoid patients.
- §To reduce tone in the psoas muscle in patients with back pain because of hyperlordosis.
- §As a simulation for orthopedic surgery, to have a general idea of how the child will be when spasticity is reduced.
 • I hope i could give you the brief overview of tone and tonal abnormalities along with use of these medications in the treatment of CEREBRAL PALSY.
• I hope i could give you the brief overview of tone and tonal abnormalities along with use of these medications in the treatment of CEREBRAL PALSY.